Directors' Blog
Te Awaroa – Voice of the River
Across Aotearoa New Zealand, many rivers are disappearing or no longer safe for fishing and swimming, and we are seriously concerned about declining river health. It seems like everyone I talk to from my generation or older had a favourite river or waterhole that they enjoyed as part of growing up as a Kiwi kid. When asked, very few them would swim in that river today – if it actually still existed. The ‘bottom line’ regulatory approach of the government’s freshwater reforms is anthropocentrically framed, and I argue, flawed.
Inspiring New Zealanders to take care of our waterways
Inspired by and drawing from mātauranga Māori, I am part of the Te Awaroa team that aspires to catalyse a national movement of New Zealanders taking action to care for their waterways. A critical strand of this effort is to understand the issue from the perspective of the river – what would the river say? What is it saying? Buoyed by Te Awa Tupua Act 2017, whereby the Whanganui River has been accorded legal personality, recognised as an ancestor and an integrated living whole which flows from mountains to sea, we seek to articulate, and then empower the Voice of the River.
In a Māori worldview, because there is only one set of primal parents, all things are related and we exist in a kinship-based-relationship with Te Taiao – the Earth, Universe and everything within it. Whakapapa is the central principle that orders the Te Taiao. Water appears early in the whakapapa, emerging while Ranginui and Papatuanuku are still locked in loving embrace:
Ā, ko Rū-nuku, ko Rū-rangi, ko Rū-papa,
ko Rū-take, ko Rū-kerekere,
Ko Rū-ngātoro ko koukou mataero, koi runga,
Koai ū-whāio, Ko Rū-ngātoro,
Ko Wai-o-nuku, Ko Wai-o-rangi,
Ko Wai-papa, Ko Wai-take, ko Manatu.
And, the Earth trembles, the Sky trembles, the Ground trembles,
the Source trembles, the intense trembles,
the resounding trembles, annoint the thin surface above,
Then numerous trembles, resounding ko Manatu, tremble, the ebbing,
the Waters of the Earth, the Waters of Heaven,
the Waters of the ground, the Source of Waters, the ebbing.
(From the writings of Wiremu Maihi Te Rangikaheke)
Taiao is considered as one, whole interconnected system, which comprises component parts – Taimoana the realm of water; Taiwhenua – the realm of land; Taitangata – the realm of living things; Tairangi – the realm of the atmosphere, parts that are never considered as discrete, individual pieces, but only ever as part of the whole, as they are inextricably linked.
Now, let me introduce you to the Tarawera River
I have been privileged to have spent time with the Tarawera and some of its people over the past decade.
At its head waters, after it flows out of Lake Tarawera, the Tarawera River is crystal clear, bursting with life, with luxuriant native bush nestling right up to its banks:

After a short 65 km journey to where it flows into Te Moana a Toi – Bay of Plenty, it changes to this:

The tragic situation that has befallen the Tarawera is not unique. Across New Zealand, many rivers are no longer safe for fishing and swimming, and Kiwis are really worried about our rivers. And those are the rivers and streams that haven’t been subjected to the abject humiliation of having been buried alive in pipes, or those that only flow sporadically, if at all, as their waters have been over-allocated for irrigation or other purposes.
Data show we are in a freshwater crisis
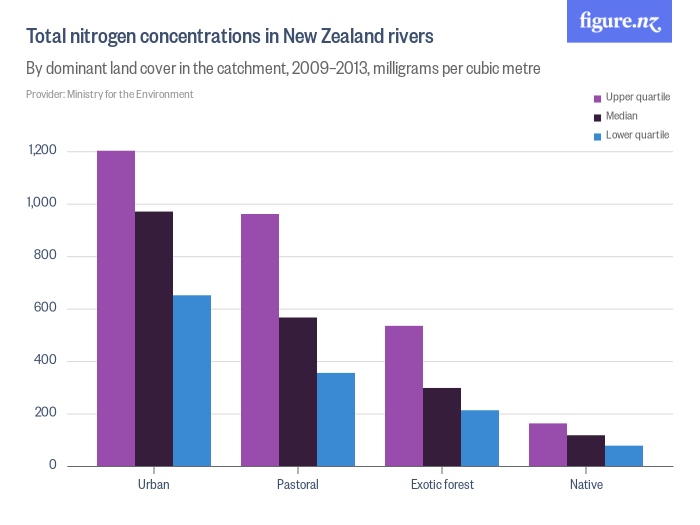
Waterways in New Zealand are in a perilous state. Research shows an alarming and overwhelming trend of degraded water quality, of lost wetlands, of exhausted or polluted aquifers and intensive catchment land modification. Whether too little, too much, or too dirty, for many years, voices articulating their fears about the decline were ignored in favour of development imperatives but more recently communities, industry, business, politicians and philanthropists have joined the chorus of concern. Some sobering statistics:
- 70% of our rivers don’t meet Ministry of Health recreational contact guidelines
- Sediment chokes many harbours and estuaries
- 90% of our wetlands gone
- 18,000-34,000 people contract waterborne diseases every year
- Pollution of freshwater is spreading

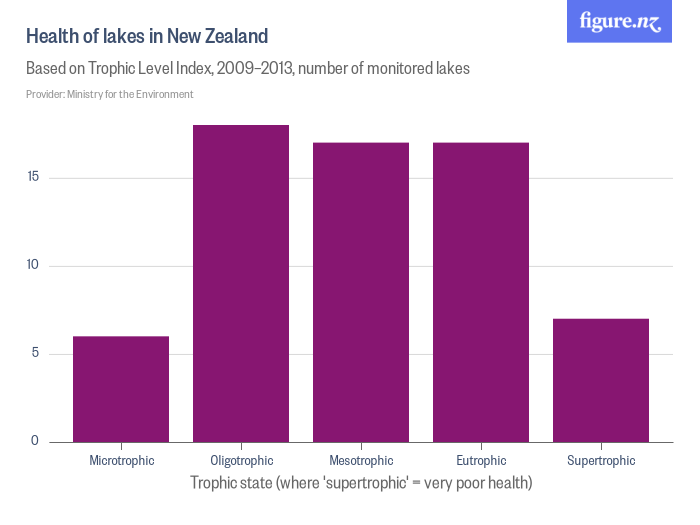
New Zealand is in a freshwater crisis. It’s not maybe, it’s not perhaps, it’s not it’s coming – we are in it.
It’s no wonder then that the OECD has told us that our growth model is approaching its environmental limits. It’s no wonder then that the state of our freshwater is the environmental issue of highest public concern.
The anthropocentrically framed ‘bottom line’, ‘humans first’ regulatory approach of the government’s strategy for freshwater, I believe, is flawed.
For example, $44 million funding to enable rivers and lakes across NZ to be improved compared with $400 million to fund irrigation Investment.
Sadly, NZ is not alone, the truth is that dominant civilisations on the planet are behaving in a way that is leading our children and our children’s children and our children’s children’s children into a bleak, unsustainable future, that most of us don’t want.
The details of what we are doing to Earth and how harmful our impacts are, are complex and some of the facts controversial, or even just being ignored. However, it is patently obvious that we humans are behaving in a manner which is destroying the Taiao. It seems that we just don’t care.
Focusing back now to NZ and its rivers, decision-makers argue about national standard parts-per-million this and dissolved oxygen limit that, missing the point entirely that in whatever techno-scientific terms and rationalisations are being used to justify the decisions – our rivers are dying.
Te Awaroa research and action project
Business as usual will condemn our waterways and with it our people, our food and recreation sources, our economies, our identity to certain death. Te Awaroa, Voice of the River, is not business as usual. Te Awaroa is a foundational Ngā Pae o te Māramatanga research and action project intent on catalyzing and inspiring a national movement of New Zealanders taking care of their waterways with a goal of 1,000 rivers in a state of ora (health) by 2050.
Te Awaroa seeks to transform New Zealanders’ relationship with rivers, founded upon a kinship relationship with Taiao, and building on practical and personal connections to foster a duty of care. Although a kinship approach is drawn from a Māori worldview and knowledge base, the idea enjoys widespread support of many Kiwis, as it is consistent with how many of us ‘feel’.
Within this framework Te Awaroa will use participatory and action research approaches along with mana whenua monitoring, maintenance and enhancement to allow the emergence of newly re-discovered and innovative approaches and tools to establish healthy relationships between a waterway and its people, animals and plants, to bring about a very different way of living with rivers.
The perception of apathy I mentioned earlier is just that, a perception. In reality, dozens if not hundreds of committed, passionate and dedicated individuals and groups are working tirelessly around Aotearoa New Zealand to achieve better outcomes for our rivers and waterways.
Reframing the issue from the river’s perspective
I learnt from the Coast Salish First Nations people of Vancouver Island that because we have two ears and one mouth, it is twice as important to listen as to speak. Inspired by that paradigm, a critical difference of the Te Awaroa effort is to reframe the issue from the perspective of the river – what would the river say? What is it saying? We seek to listen, then articulate, and then empower the voice of the river, drawing from all knowledge available.
We seek to understand river health: what the water quality is – nutrients, sediments, pathogens, human, animal and industrial waste and whether there is enough water for the flora and fauna to thrive.
We seek to understand river behavior: the underlying geology, fluvial geomorphology, flooding. When a river floods, it is a river behaving like a river.
We seek the rivers’ stories – how we know the river – from multiple views and perspectives. Ko au te awa, ko te awa ko au.
I believe that two of the key reasons why there is not more widespread condemnation of current unsustainable practices and action is that everyday people:
- Do not have relationships with waterways anymore – it’s hard to care about something you don’t have a relationship with, and
- Feel a sense of powerlessness in the face of the relentless machine that continues to take and take and take.
Therefore, the aim of the Te Awaroa Voice of the River approach is to reintroduce people to their waterways, to rekindle those relationships, by exploring whakapapa, sharing river narratives, making hikoi along rivers, articulating the voice of the fish, the eels, the algae, the macroinvertebrates, the behaviour of the river. Collectively, these ‘voices’ constitute the ‘Voice of the River’.
One of the few exceptions to the constant onslaught being wrought on our waterways is Te Mana o te Wai – a section of the National Policy Statement on Freshwater Management that flows out of a Māori kinship framing and mātauranga Māori. It asserts that water is a taonga to Māori and it carries mauri. This is reflected in the concept of Te Mana o te Wai – the innate relationship between te hauora o te wai (the health and mauri of water) and te hauora o te taiao (the health and mauri of the environment), and their ability to sustain te hauora o te tāngata (the health and mauri of the people)”.
In effect, this approach says – first, it is the right of a river to be a river, second, we need to ensure the integrity of the catchment and flora and fauna, and third, only then can humans seek to derive sustenance.
Daniel Hikuroa
About:
Dr Daniel (Dan) Hikuroa, a Principal Investigator at Te Pūnaha Matatini, is an earth systems scientist at the University of Auckland who integrates mātauranga Māori (Māori knowledge) and science to realise the dreams and aspirations of the communities he works with. Dan’s many projects include the co-writing of the 2014 State of the Hauraki Gulf Environment Report.
What is WaiNZ?
Kia ora, Aotearoa. We’ve asked leading environmental, social and health researchers to share their personal and professional perspectives about the state of our water and what water means to us as New Zealanders. Follow their blogs right here at tepunhahamatatini.ac.nz and across social media with #WaiNZ.
Where possible, commentary will be backed up by data from Figure.NZ. Their incredible charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #WaiNZ data board and sign-up to create your very own data board on any topic that interests you.

Nau mai haere mai ki WaiNZ
Kia hiwa ra! Kia hiwa ra!
Kia hiwa ra i tēnei tuku, kia hiwa ra i tērā tuku!
Kia hiwa ra! Kia hiwa ra!
E ngā waka. E ngā hau e wha. E ngā mana. E ngā iwi.
E ngā manu kōrero o runga i ngā marae.
Whakarongo! Whakarongo! Whakarongo!
Ki te tangi a te manu e karanga nei “Tui, tui, tuituia!”
Tuia i runga, tuia i raro, tuia i roto,
Tuia i waho, tuia i te here tangata.
Ka rongo te pō, ka rongo te pō,
Tuia i te kawai tangata i heke mai i Hawaiki nui,
i Hawaiki roa, i Hawaiki-pamamao,
i hono ki te wairua, ki te whai ao, ki te Ao Mārama.
Tihei Mauriora!
Be alert! Be watchful!
Be alert on this rampart! Be alert on that rampart!
Be watchful! Be alert!
O the canoes. The four winds. Great ones. The tribes.
Orators of the marae.
Listen! Listen! Listen!
Listen to the cry of the bird calling “Unite, unite, be one!”
Unite above, unite below, unite within,
Unite without, unite in the brotherhood of man.
The night hears, the night hears,
Unite the descent lines from Great Hawaiki,
From long Hawaiki, from Hawaiki far away,
Joined to the spirit, to the daylight, to the world of light.
E ngā mana, e ngā reo, e ngā karangatanga maha ka tuku mihi nui ki a koutou, ki a tātou katoa, i raro o te āhuatanga o Mahuru Māori me te wiki o te reo Māori. Nō reira, nau mai, nau mai, haere mai. Haere mai ki tēnei kaupapa, ko WaiNZ.
Ko WaiNZ tētahi wānanga ipurangi mā ngā kairangahau me ngā kaimahi ki roto o tēnei kaupapa, kia puta mai ai i ā rātou kōrero, i ō rātou whakaaro, i ō rātou moemoea e pā ana ki te taonga nei, te wai.
The great ones, the spokespeople, the many, best wishes to you, to us all, under the auspices of Mahuru Māori and Māori Language Week. Therefore, welcome to this campaign, WaiNZ.
WaiNZ is a platform for thinkers and doers in this space, to share their stories, their thoughts, their dreams for our treasure – water.
Herein we will explore people’s personal and professional relationships with water to highlight the importance of protecting and cherishing our waterways for health, social, economic, cultural and environmental reasons.
WaiNZ will comprise a week-long online conversation with blog posts and other media from influencers and researchers who work on ‘ngā ahuatanga katoa o te wai; mai ngā maunga ki ngā moana, mai ngā puna ki ngā pūahatanga, mai ngā tōuarangi ki ngā tai – all aspects of water, from the mountains to the oceans, from the springs to the harbours, from the rain to the sea.
This whakatauki expresses the importance of water, and embodies the force driving WaiNZ:
“Ko te wai te ora o ngā mea katoa – Water is the life giver of all things”
In a Māori worldview because there is only one set of primal parents, all things are related and we exist in a kinship-based-relationship with Te Taiao – the Earth, Universe and everything within it. Whakapapa is the central principle that orders the Te Taiao. Water appears early in the whakapapa, emerging while Ranginui and Papatuanuku are still locked in loving embrace:
Ā, ko Rū-nuku, ko Rū-rangi, ko Rū-papa,
ko Rū-take, ko Rū-kerekere,
Ko Rū-ngātoro ko koukou mataero, koi runga
Koai ū-whāio, Ko Rū-ngātoro,
Ko Wai-o-nuku, Ko Wai-o-rangi
Ko Wai-papa, Ko Wai-take, ko Manatu.
And, the Earth trembles, the Sky trembles, the Ground trembles,
the Source trembles, the intense trembles,
the resounding trembles, annoint the thin surface above,
Then numerous trembles, resounding ko Manatu, tremble, the ebbing,
the Waters of the Earth, the Waters of Heaven,
the Waters of the ground, the Source of Waters, the ebbing.
(From the writings of Wiremu Maihi Te Rangikaheke)
Nō reira, nau mai, haere mai ki tēnei haerenga ki te whakatewhatewha o ngā moemoea, ngā wawata, ngā pātaitaingia o maha ngā mea e pa ana te wai. Ko tō māua tumanako, mai a WaiNZ ka puaki te hā o te wai.
Therefore, welcome and join us on this journey of exploration of the dreams, the aspirations, the many challenges facing water. It is our hope that through WaiNZ, the voice and essence of the water will emerge.
Whano, whano! Haramai te toki! Haumi ē! Hui ē! Tāiki ē!
Dan & Siouxsie
About:
Dr Daniel (Dan) Hikuroa, a Principal Investigator at Te Pūnaha Matatini, is an earth systems scientist at the University of Auckland who integrates mātauranga Māori (Māori knowledge) and science to realise the dreams and aspirations of the communities he works with. Dan’s many projects include the co-writing of the 2014 State of the Hauraki Gulf Environment Report.
Dr Siouxsie Wiles is Deputy Director (Outreach and Public Engagement) of Te Pūnaha Matatini. She describes herself as a microbiologist and bioluminescence enthusiast. As Head of the Bioluminescent Superbugs Lab at the University of Auckland, Siouxsie combines her twin passions to understand the interplay between environment and infectious diseases.
What is WaiNZ?
Kia ora, Aotearoa. We’ve asked leading environmental, social and health researchers to share their personal and professional perspectives about the state of our water and what water means to us as New Zealanders. Follow their blogs right here at tepunhahamatatini.ac.nz and across social media with #WaiNZ.
Where possible, commentary will be backed up by data from Figure.NZ. Their incredible charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #WaiNZ data board and sign-up to create your very own data board on any topic that interests you.
Maths Craft Festival arrives in Auckland
Do you enjoy craft? Then you probably enjoy mathematics too – you just may not know it yet. Don’t miss out on Maths Craft Festival 2017 being held this coming Saturday and Sunday, September 9-10, at the Auckland Museum.
Discover the maths behind craft and the craft behind maths. Find out how to tie a mathematical knot, crochet a Möbius strip, fold an origami octahedron, draw an impossible triangle, or colour a Latin square.
Ten craft creation stations will be set up in the museum’s event centre, a fully glazed circular room on top of the museum roof. Featuring incredible views of the city and harbour, it also has plenty of natural light – perfect for crafting. And there will be lots of space and seating, so you can stay and craft all day!
Sharing the beauty of maths
Dr Jeanette McLeod and Dr Phil Wilson, senior lecturers at the University of Canterbury’s School of Mathematics and Statistics, will lead a team of volunteers and host the two-day festival, part of a nationwide tour to raise interest in maths among New Zealanders.
“By using craft as a medium… we aim to introduce adults and children alike to a new and fun way of engaging with mathematics,” says Dr McLeod.
“Through these events, we’re keen to show people how maths underpins almost every aspect of today’s society. Whether it’s used in crafts, technology, business, science, social science or education, maths is vital,” she says.

Learn how to make an origami icosahedron (pictured) and many other wonderful creations at this weekend’s Maths Craft Festival.
Dr McLeod has crocheted and knitted a variety of mathematical objects – from Möbius strips to intricate coral-like hyperbolic planes – and is passionate about sharing maths as the language of science. Her specialisation is combinatronics, with a particular focus on asymptotic enumeration, graph colouring, random graphs, and Latin squares. She is also an accomplished crafter and crocheter.
Dr Wilson, who usually works in the field of theoretical fluid dynamics and mathematical modelling in biology and industry, says Maths Craft Festival offers something for everyone.
“A lot of our speakers are really good at finding mathematics in ordinary everyday things –from how you tie your shoe laces, tie knots or even how to set a wobbly table straight,” says Dr Wilson. “Maths Craft is really for all ages and all backgrounds.”
Public talks promise to fascinate
The two-day festival will also include five public talks over the course of the weekend:
- Associate Professor Clemency Montelle, University of Canterbury – The (a)symmetry of a sari (September 9, 2.30pm)
- Ms Elizabeth Chesney, University of Canterbury – Knuts about knitting knots (September 9, 3.45pm)
- Associate Professor Burkard Polster, Monash University – What is the best way to lace your shoes? (September 9, 5.15pm)
- Dr Michael Assis, University of Melbourne – The beauty of origami / The beauty of mathematics – connecting folds (September 10, 2.30pm)
- Professor Bernd Krauskopf and Professor Hinke Osinga, University of Auckland – Chaos in Crochet and Steel (September 10, 3.45pm)
Where and when?
Maths Craft Festival is being held at the Auckland War Memorial Museum Events Centre on Saturday 9 September and Sunday 10 September. All are welcome and entry is free with a museum ticket. Maths Craft is running a free bus service from South Auckland to the Museum on Sunday 10th September (see www.mathscraftnz.org/events/maths-craft-festival#bus-service for details of how to book your free seat).
Visit the Maths Craft website for more information about upcoming events in Dunedin: www.mathscraftnz.org. Also on Facebook, Ravelry, and Twitter #mathscraftnz

#WaiNZ – Let’s talk about our water
New Zealanders have heard a lot about the state of our waterways and water in recent months. With the 2017 General Election just around the corner, politicians, industry insiders, communities and researchers have clamoured to get their views and policy ideas into the public arena.
Clarity is needed to inform policy decisions
While there is general agreement that our water is a precious resource, certain issues – such as how to protect it from pollution and the application of a tax for commercial users – have become contentious.
Dr Daniel Hikuroa, associate investigator at Te Pūnaha Matatini Centre of Research Excellence and an earth systems scientist who integrates mātauranga Māori (Māori knowledge) with science, says it’s time that we all gained some clarity on the issue so we can inform relevant policy.
“This means not only examining the scientific evidence, but finding out what water means to us as a people, our wairua and for Aotearoa,” says Dr Hikuroa.
“We want to explore people’s personal and professional relationships with water to highlight the importance of protecting and cherishing our waterways for health, social, economic, cultural and environmental reasons.”
Dr Hikuroa and prominent microbiologist Dr Siouxsie Wiles, deputy director of Te Pūnaha Matatini, are running WaiNZ – an online campaign from 11-15 September that aims to bring the role and state of water in Aotearoa New Zealand to the forefront of national consciousness.
Data infographics to underpin the conversation
The week-long conversation will provide New Zealanders with an opportunity to read blog posts and other media from key influencers who will talk about their relationships with water, while drawing on research data and a multitude of charts provided by Figure.NZ.
“The end result will be a mix of data-driven and personal stories that form an online curated conversation, underpinned by easy to understand data visualisations,” says Dr Wiles.
“We want to help shape a data-driven conversation to better understand what is happening to our water and find out how everyone – the general public, the agricultural sector and policymakers – can work together to conserve it for the future.”
Join in the conversation on Twitter!
If you’re interested in taking part in this important national conversation about water and our waterways, then follow the #WaiNZ campaign on Twitter or in the mainstream media during the week of 11-15 September.

Sexism and the gender pay gap – data that can’t be ignored
A recent study by researchers at Motu Economic and Public Policy Research provides strong, definitive evidence that sexism is mostly to blame for the gender pay gap in New Zealand.
The study found that, on average, women in New Zealand’s workforce are paid 84 cents for every $1.00 a man earns, despite there being no statistically significant difference in productivity levels between male and female employees.
“This study is different to most previous wage gap studies in that it tests whether men and women are paid different wages for adding the same amount of value to their employer,” said lead researcher Dr Isabelle Sin, Fellow at Motu and Principal Investigator at Te Pūnaha Matatini.
Motu study dispels some common arguments

Lead study researcher Dr Isabelle Sin, Fellow, Motu Economic and Public Policy Research and Principal Investigator, Te Pūnaha Matatini.
The researchers analysed New Zealand tax data for 50 per cent of the working population from 2001 to 2011, to determine how much of the overall difference between women and men’s pay could be attributed to women being employed in industries that pay less.
“We found that women were over-represented in low-paying industries like food and beverage services, but this explains a mere 7 per cent of the entire gender wage gap,” Dr Sin said. “If you add in the fact that women also tend to work in low-paying firms, we can say that 12 per cent of the overall gender wage gap is due to the particular industries and firms where women work.”
The study then looked at productivity and wages of New Zealand men and women in private, for-profit organisations with five or more employees. Using employee-level data linked to business information, they found that on average, Kiwi women are paid 16 per cent less than their male counterparts for making a contribution of the same value to their employer.
Overall, the data suggest that sexism is a drag on large segments of New Zealand’s economy, with the gender wage-productivity gap as high as 40 per cent in some sectors – in finance and insurance, telecommunications, transport equipment manufacturing, water and air transport, and electricity, gas and water, and rail.
“It’s worth noting that these are all sectors that have the potential for monopoly-created profits and have low competition,” said Dr Sin. “To put it simply, our research suggests sexism is likely to be a major driver of the gender wage gap. What we’re going to do about it is another matter.”
NEW paper: women & men add same value to their firms, but average woman paid only 84 cents for every $1 for average man. pic.twitter.com/chAMk1fAXd
— Motu Research (@moturesearch) August 28, 2017
Quality of the data make findings difficult to ignore

Professor Tava Olsen, Deputy Director – Industry and Stakeholder Engagement at Te Pūnaha Matatini.
Professor Tava Olsen from the University of Auckland, Director at the New Zealand Centre for Supply Chain Management and Deputy Director, Industry and Stakeholder Engagement at Te Pūnaha Matatini, described the results as “pretty definitive”.
“There is a gap and [because the study researchers] were able to get firm-level data on productivity, there’s really no explanation for it other than implicit bias or sexism,” said Professor Olsen.
The Motu research is a lot harder to ignore than previous studies due to its sheer size and the nature or quality of the data collected, she added.
“It’s not until you get a really big study like this that you can say ‘Oh yes, there is actually a problem here.’ Obviously, this isn’t the first study to show gender pay gaps, it’s just a very clean one in terms the data they got access to,” she said. “I doubt there are many countries who allow researchers access to their tax data… If you think about it, it’s pretty phenomenal.
“So I think this is quite important research in terms of showing there is a real gap. There is a problem here and it’s not really okay,” said Professor Olsen.
“Hopefully, companies will start putting procedures in place to check themselves and try and start looking at their own gender gaps.”


Te Pūnaha Matatini supporting NZ science journalism
Te Pūnaha Matatini is a major contributor to the Aotearoa-New Zealand Science Journalism Fund, which recently awarded $20,000 in funding to several New Zealand science journalists to cover stories ranging from genomics to driverless vehicles to climate change.
This first round of funding received 20 applications, with six projects involving journalists from a variety of media outlets across the country being selected.
“Overall, we were extremely impressed with the range and quality of the applications – from established science journalists to relative newcomers, from a range of media and from around the country,” said the fund’s founder Dr Rebecca Priestley.
We’re delighted to announce first round of funding! We had 20 applications and have funded 6 projects https://t.co/ANuD79A5Id 1/8
— NZ Sci Journalism (@scijournofund) August 20, 2017
Controversial technologies to be covered
Within the fund’s category on ‘Controversial technologies: Should we even go there?’ Te Pūnaha Matatini is funding three projects to a total of $10,000, as follows:
- $4,500 to Naomi Arnold (New Zealand Geographic article)
- $4,000 to Simon Morton (RNZ’s This Way Up feature)
- $1,500 to William Ray (RNZ’s Our Changing World series)
All of the projects are expected to be published by the end of 2017, after which they will be available under Creative Commons licence. Science journalists from around New Zealand will then have a second opportunity to apply for funding through the Aotearoa-New Zealand Science Journalism Fund in early 2018.
“Round one showed that journalists want to work on important science-related stories and that there is appetite to fund them doing so,” said Dr Priestley. “We are looking forward to seeing these projects come to fruition and to working on securing funding for round two.”
How to support the Aotearoa-New Zealand Science Journalism Fund
Interested readers and organisations wishing to support the fund can do so by emailing Dr Rebecca Priestley at sciencejournalismfund@gmail.com or through the Aotearoa-New Zealand Science Journalism Fund Press Patron crowd-funding page.

Dr Rebecca Priestley wins Prime Minister’s Prize – fourth for Te Pūnaha Matatini
Te Pūnaha Matatini investigator Dr Rebecca Priestley has been announced as the winner of the 2016 Prime Minister’s Science Communication Prize.
Dr Priestley is a senior lecturer at Victoria University of Wellington in the Science in Society Group. She has been an Associate Investigator in Te Pūnaha Matatini since the Centre was established in 2015.
Te Pūnaha Matatini is one of ten national Centres of Research Excellence. Its research focuses on the science of complex systems and networks, and applies this to study problems in society, the environment, and the economy. Dr Priestley co-leads a project in the Centre that studies public engagement by researchers.
“Dr Priestley is unique amongst New Zealand’s science communicators”, says Prof Shaun Hendy, Director of Te Pūnaha Matatini. “She is not only an accomplished science writer and journalist, she also has academic standing as one of New Zealand’s leading historians of science and has undertaken pioneering work in the study of science’s engagement with society.”
She received the $100,000 prize from the Prime Minister at an event in Wellington today, joining Te Pūnaha Matatini’s Dr Michelle Dickinson, Dr Siouxsie Wiles and Prof Hendy, as previous winners of the prize.
“We’ve placed public engagement and communication of our research at the heart of our mission” added Hendy, “and so it should be no surprise that Te Pūnaha Matatini has become the meeting place for New Zealand’s leading science communicators.”
Some of Dr Priestley’s prize money will be used to establish New Zealand’s first fund to support science journalism. Te Pūnaha Matatini will also contribute to this fund.
“As newsrooms shrink, it is getting harder for the media to cover science,” says Hendy. “For science engagement to work well, journalists need to be able to take the time to cover science stories critically. We hope this fund will help sustain independent science journalism in New Zealand.”
Contact: Dr Rebecca Priestley (Rebecca.priestley@vuw.ac.nz 021 917050); Prof Shaun Hendy (shaun.hendy@auckland.ac.nz 021 1442349)

Taking a stand for science and society
The world has taken a horrible turn for the worse in the last few weeks. Following a rather bizarre inauguration weekend that featured a running dispute over the size of Trump’s crowd and then the inspiring Women’s March, the Trump Administration unsettled the world with a flurry of controversial orders, some likely illegal and most certainly immoral. I did not expect to see things go this wrong, this fast.
The travel bans were probably the most frightening in intent, blocking people from travelling to the US on the basis of their place of birth, including existing legal residents as well refugees who were on the verge of making a new start. The orders themselves were drafted to avoid the overt racism and hostility towards Muslim society that characterised the Trump campaign, but failed in this by their construction on the flimsiest of pretexts. It was a dog-whistle that everybody could hear.
The impact on many people, including those fleeing wars in Syria and Yemen, was immediate. Around the world students, refugees, and others in vulnerable circumstances were turned away or detained at airports, separated from their families, or saw their hopes for escaping deadly conflict destroyed.
Te Pūnaha Matatini is the meeting place of many faces, and amongst our diverse community are friends and colleagues who have been directly affected by this ban. Just as we would not tolerate a researcher who refused to work with people on the basis of their place of birth, their gender, or their religious beliefs, we also have no tolerance for politicians who craft policies that use this as a basis to single out vulnerable people for harm.
What can we do? At Te Pūnaha Matatini HQ we’ve been writing to people in positions of power to urge them to take a stand. If you’d like to know how we’ve been going about this, then drop us a line.
We will also be supporting the March for Science, which will take place on Earth Day, April 22. The focal point for the March will be Washington DC, but there will also be marches in cities in New Zealand. You can follow @ScienceMarch_NZ on twitter if you would like to join in here in New Zealand.
This march is not just for scientists. The Trump administration has already sent strong signals that it is willing to hinder the science community’s ability to speak to the public and it is highly likely that cuts to science funding will follow. Climate change and the degradation of the environment will affect everyone, however, and it is the already marginalised who stand to lose the most. And none of the crises that society faces today are solvable unless we also address social injustice.
I’ve seen and heard comments that politics has no place in science, but these remind me of what I heard when New Zealanders marched against the Springbok Tour in 1981. One must acknowledge that science flourishes under some political arrangements, while it fails under others. When politicians abandon tolerant discourse, respect for others, and dismiss the value of evidence, science is in trouble. Whose job is it then to ensure the public understands this, if not the science community?
I’ve also seen pleas from some scientists to be left alone in their labs to get on with their science; some high profile scientists have argued that by addressing intersectionality, the march organisers are also attempting to put politics into science. We know that in science itself there are inequities and power structures that prevent or make it harder for some groups of people to become scientists in the first place. Only the most privileged in our society have labs in which to hide. There is no equivalence between the politics of Trump that seeks to exclude, and the efforts of many scientists to make science accessible to everyone.
Shaun Hendy is Director of Te Pūnaha Matatini. In 2016 he authored the book Silencing Science which explores the public obligations of scientists and instances where scientists have been prevented from speaking out.

Scholarship established following “Hidden Figures” gala screening
A fundraising campaign and gala screening of the critically acclaimed film Hidden Figures has raised $13,500 to help establish a scholarship for women to study physical sciences, maths or engineering in 2018.
Te Pūnaha Matatini’s Executive Manager Kate Hannah, Deputy Director Dr Siouxsie Wiles and University of Auckland Associate Professor Nicola Gaston from the Department of Physics organised the fundraising campaign to raise the profile of Māori and Pacific female scientists and students.
Listen to an interview with Kate Hannah on Radio Zealand’s Morning Report:
In addition to funds raised through the Givealittle campaign, five New Zealand Centres of Research Excellence provided financial contributions toward the scholarship: Te Pūnaha Matatini, the Dodd-Walls Centre for Photonic and Quantum Technologies, the MacDiarmid Institute for Advanced Materials and Technology, the Maurice Wilkins Centre, and Brain Research New Zealand. The University of Auckland Department of Physics also contributed.
The scholarship will be administered by the Association for Women in the Sciences (AWIS).
20th Century Fox, EVENT Cinemas, SOHO Wines and L’Oreal New Zealand provided valued assistance and promotional material for the gala screening of Hidden Figures.
Donate to an ongoing scholarship fund to support women in New Zealand science.
Read more:
- Scientists raise $13k for women to study – Radio New Zealand
- Q+A: NZ science’s own ‘Hidden Figures’ – New Zealand Herald
- Hidden Figures movie trailer – 20th Century Fox
- Te Pūnaha Matatini’s commitment to diversity, our sponsorship policy, and event code of conduct.
Analytics to improve health delivery systems
Te Pūnaha Matatini Associate Investigator Dr Michael O’Sullivan discusses analytics to improve health delivery systems.
Michael researches a combination of Operations Research and Analytics and is a Senior Lecturer at the Department of Engineering Science and the Precise, and Timely Healthcare Theme Leader at the Precision Driven Health Research Partnership. The latter is a data science research initiative that features collaborations between the University of Auckland and partners in the public, corporate and healthcare sectors.
This presentation was recorded at an Orion Health Seminar on 6th December, 2016.