Directors' Blog
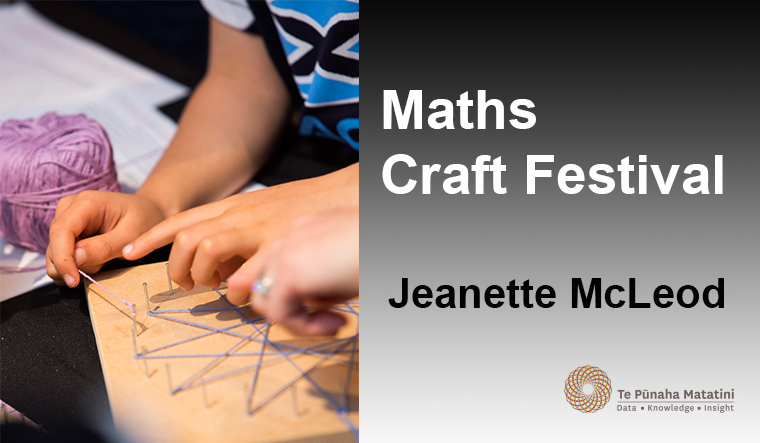
Maths Craft Festival
Enjoy craft? Then you probably enjoy mathematics too, you just may not know it. This was the idea behind the recent Maths Craft Festival, a weekend-long festival held at the Auckland Museum, celebrating the many links between mathematics and craft. The Festival was the creation of Jeanette McLeod (University of Canterbury/Te Pūnaha Matatini) and Julia Collins (University of Edinburgh), who were inspired to start the festival after a serendipitous encounter while Julia was on holiday in Christchurch. Jeanette and Julia – both avid knitters and crocheters – wanted to find a way to share the beautiful mathematics behind craft with the public. Jeanette pitched the idea to Te Pūnaha Matatini who responded with instant enthusiasm, and not only offered to be the major sponsor, but encouraged Jeanette and Julia to “think big”. With that, the idea of the Maths Craft Festival was born. A short time later, after being coerced into crocheting a hyperbolic plane, Phil Wilson (University of Canterbury) was recruited. Together the trio went on to create the first event of its kind in New Zealand.
The Festival combined eight hands-on craft stations with a series of public talks, and was immensely popular, even making an appearance on One News. Over 1,800 people visited the Festival, trying their hands at a range of mathematical crafts, including crocheting hyperbolic planes, building fractal sculptures, making Möbius strips and folding origami dodecahedrons. The public talks were given by mathematicians and crafters, and covered topics ranging from the mathematics of knitting, and the Four Colour Theorem, to fractals in art and nature, and chaos and the crocheted Lorenz Manifold. (In fact, Prof Hinke Osinga issued a challenge during her talk: be the first in NZ to crochet a Lorenz manifold and she will send you a bottle of champagne.) The Festival was the largest event run at the Museum in over six months, and was praised by staff for not only its popularity, but for attracting a such diverse group of people.
The Festival was an experiment, born of a desire to share the beauty of the mathematics in crafts, and it really hit a nerve. The positive feedback was overwhelming, with comments like “What a great event, our whole family has enjoyed it, from age 7-47!” and “Thank you for putting up such a cool event! Math is awesome.” Others thought that it was “Brilliant to see so many people old and young being enthused by mathematics. Let’s hope more of these events happen as there is clearly high demand for more maths related fun.” School teachers were inspired and “Have come away with some fabulous ideas to share with numerous teachers and their classrooms across Auckland. Looking forward to this becoming a regular event …. hint, hint.” In fact, the most common piece of feedback can be summed up by this comment: “Loved it, please repeat!”
What did people learn from attending the Festival? Aside from experiencing the “fascinating complexity and depth to all of the various constructions”, they were “amazed by how much breadth mathematics encompasses”, and have now come to realise that “Fractals are EVERYWHERE” and “Geometry is way cool.” And perhaps most heartening of all, that “Maths is exciting” and “maths can be fun!”
The Festival has proved to be so popular that Auckland Museum have asked for it to be run again next year – in their Events Centre, the copper dome on the roof of the museum with a 360-degree view over Auckland and space for 500 people. Plans are also underway to take Maths Craft on the road in 2017, and run events in other parts of New Zealand.
For more information on the Maths Craft Festival, or in case you’re yearning to fold an origami dodecahedron or crochet a hyperbolic plane, please visit mathscraftnz.org.
The Maths Craft Festival couldn’t have happened without the help and support of Shaun Hendy, Kate Hannah, Sarah Hikuroa, Danene Jones, Nicolette Rattenbury, Sarah Mark, Andrea Webley and the Auckland Museum, and our generous sponsors Te Pūnaha Matatini, the University of Canterbury, the University of Auckland, the New Zealand Mathematical Society, the Dodd-Walls Centre and Ashford.
InfectedNZ – Twitter Q+A
Did you miss our InfectedNZ campaign with Figure.NZ? Don’t worry – we’ve put together a collection of resources and Twitter Q+A to help answer your burning questions.
Resources
- InfectedNZ blogs
- Science Media Centre – Antimicrobial resistance – expert Q+A
- Science Learning Hub – teacher and student-orientated information about fighting infections, the immune system, and the work of some researchers.
- NZ Herald online“The big read: is the world on the brink of an antibiotic apocalypse?”
- The Spinoff “In the fight against the superbug apocalypse, don’t fall for the idea that infectious diseases only happen somewhere else.”
- Newshub. “Online campaign highlights dangers of infectious diseases.”
- Newshub. “Antibiotics will soon stop working, scientists warn.”
- NewstalkZB “Antibiotic resistance a growing threat to world health.”
- The Spinoff “Calling a vagina a vagina: why cutesy code words are terrible for our sexual health.”
- Waikato Times “Urgent action needed to combat killer infections.”
Twitter Q+A
Reception for Women in Mathematics and their Supporters at NZ Mathematics Colloquium
After the AGM for the New Zealand Mathematical Society on Monday 5th of December, there will be a reception for women in mathematics and their supporters. Everyone is welcome. The reception is sponsored by Te Pūnaha Matatini and will be chaired by Principal Investigator Dion O’Neale.
The event theme is: Being an ally: what we can all do to improve equity.
Abstract: Advocating for improved equity is a task that often falls to members of under-represented groups. This is problematic for a number of reasons; not least because it means that some of the voices that most need to be heard are least numerous and are, perhaps, undermined by perceptions of self-interest.
This event will begin with some background on what it means to be an ally, the benefits it can bring, and some of the potential pitfalls that can be associated with it. Over drinks, we will discuss the things that we can all do as individuals, both at work and at home, in order to improve equity in our departments and the New Zealand mathematical sciences community.
This event comes with a code of conduct: see http://nzmathsoc.org.nz/downloads/miscellaneous/CodeOfConduct-NZMC-WiM.pdf?t=1479095141.
SciGlow at Silo Park: the art of bioluminescent bacteria
Be wowed by the eerie glow of bioluminescent bacteria as art and science unite for SciGlow at Silo Park Auckland, 3-4 December.
Microbiologist Dr Siouxsie Wiles has teamed up with artists, schoolchildren and bioluminescent bugs to create the unique bacterial paintings in giant petri dishes. View intriguing artworks by professional artists or try your own hand at creating a living, glowing masterpiece.
Proudly sponsored by the Maurice Wilkins Centre for Molecular Biodiscovery, Te Pūnaha Matatini and the University of Auckland.
Dates: December 3-4
Time: 11am-6pm
Where: Silo Park, Auckland
Cost: Free

We take antibiotics for granted at our peril
I am an ardent defender of people being free to choose what they do with their own life, even when I would not make the same decision. Partly this is because studying economics gave me an appreciation of how individual decision making is surprisingly effective at producing good outcomes, and partly it is me following the golden rule: I don’t like people telling me what to do so I try to refrain from telling others what to do.
I make an exception when it comes to antibiotic use.
The difference being that most health choices that people make primarily affects themselves. However, when people misuse antibiotics this presents a direct threat to my health. Misuse increases the risk of bacterial resistance to antibiotics which compromises the effectiveness of treatments I may need in the future. In economics, we call this an externality – when the choice an individual makes has a direct flow on effect to a third party. When externalities are present the result of individual decision making is not likely to be the best possible outcome.
When it comes to antibiotics there are a number of ways in which individual decision making is clearly causing bad outcomes. When people demand antibiotics to treat illnesses that do not require it, they are not considering the contribution their unnecessary use will make to future resistance. One more person taking antibiotics won’t make much of a difference, right? And if it helps this pesky cold go away then so be it!
Thankfully, in New Zealand we do have safeguards in place to mitigate overuse. Antibiotics are only available by prescription from a medical professional. This is a major step in combatting overuse that could occur if patients were able to self-medicate. Sadly, many countries do not have these responsible safeguards in place and overuse is rampant.
Doctors who are too willing to prescribe antibiotics to placate patients are part of the problem. The Center for Disease Control and Prevention estimates that one in three prescriptions for antibiotics in the US are unnecessary. Monitoring prescribing behaviour by doctors is important to ensure responsible prescription behaviour is taking place.
Incorrect usage after prescription is another issue. For example, people who stop taking antibiotics before finishing the prescription increase the risk of bacteria developing resistance to antibiotics. It is not easy to prevent this from happening but the government can take an active role in education campaigns to inform and persuade the public to use antibiotics correctly.
Agricultural usage is also a major concern. Antibiotics can play an important role in reducing bacterial disease in farm animals, especially important for animals living in cramped conditions which are particularly susceptible to outbreaks. However, the use of antibiotics at the farm contributes to growing resistance. Regulation to monitor agricultural usage is critical. So too is regulation to ensure farm conditions are suitable to limit the risk of disease. Consumers can also help here by choosing to purchase free-range eggs and meat, or reducing their consumption of animal products.
Antibiotic resistance is a looming threat that could have far-reaching and deadly consequences. A world where we cannot rely on antibiotics to treat infections is a very scary thought but a very real possibility if we do not take action. We take antibiotics for granted at our peril.
There are many things that both the public and the government can do to combat antibiotic resistance, but the first step is to raise awareness. Campaigns like Antibiotic Awareness Week and InfectedNZ are crucial to addressing this growing problem.
So when it comes to most health choices individuals make, I’m happy to live and let live, even when the choices may not seem like a good idea to me. But when it comes to antibiotics, I want a firm regulatory hand of government to ensure responsible use. My future health may depend on it.
About
Dr Rachel Webb is a research fellow at the New Zealand Initiative. She has a PhD in economics from the University of Canterbury, specialising in the area of health economics.
What is InfectedNZ?
Hey, Aotearoa. It’s time we had a chat about infectious diseases and what we’re going to do about the looming antimicrobial armageddon. That’s why we’ve asked leading health, social and economic researchers, and people with personal stories, to help us get real about our vulnerability and discuss solutions. Follow their blogs right here at tepunahamatatini.ac.nz and watch the conversation spread across social media with #infectedNZ.
Backing it all up, wherever possible, is data from the good folk at Figure.NZ. Their super duper charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #infectedNZ data board and sign-up to create your very own data board on any topic that floats your boat.
What the NZ science system is doing to combat infectious disease
Two years ago, to commemorate the 300th anniversary of the original Longitude Prize, the UK government offered a ten million pound prize for the solution of a significant global problem. The original Longitude prize was set up in the eighteenth century by the British Admiralty to tackle the difficult problem that mariners faced of determining their longitude at sea. Three centuries later, it was decided that the challenge addressed by new prize would be chosen by the British public by popular vote.
Voters were asked to chose between challenges such as “How can we fly without damaging the environment?” and “How can we ensure everyone has nutritious sustainable food?”. In the end, the public chose to fight the rise of antibiotic resistance in bacteria: the first team “to create a cost-effective, accurate, rapid, and easy-to-use test for bacterial infections that will allow health professionals worldwide to administer the right antibiotics at the right time” will win the prize, provided this occurs before a cut-off date of 2019.
In New Zealand we held the Great New Zealand Science Project (don’t bother googling it, as the site will now try to sell you the services of a personal trainer “Effective Personal Workouts? That’s not Rocket Science !!?!”). The 2012 campaign encouraged the New Zealand public to vote for a range of science challenges and, like the people of the UK, the public voted for a project for “Fighting Disease”. I’ve always found it remarkable that of the ten National Science Challenges that were chosen by the government, not one tackles infectious disease.
In the end there were four challenges that involved the health sciences: “A Better Start”, “Healthier Lives”, “Aging Well”, and “High-Value Nutrition”. The Healthier Lives Challenge, which at first glance seem best placed to tackle infectious disease, addresses what it calls four of New Zealand’s main non-communicable diseases: “Cancer, Cardiovascular disease, Diabetes and Obesity”. The Better Start Challenge grapples with obesity, learning, and mental health problems in children and teenagers. Aging Well concerns “brain and body health”, as well as ways “to reduce disability and moderate the impact of age-related illness such as dementia, stroke, depression and frailty.”
So despite a mandate from the public, the National Science Challenges shied away from taking on infectious disease. The report of the panel that selected the Challenges noted that research into infectious disease did not meet their threshold for additionality (that is, what would a science challenge add to the health science sector) or for current scientific capacity in New Zealand. To appraise these comments, we need to look at what else is going on in the health science system.
With that in mind, the other major source of health science funding in New Zealand is the Health Research Centre (HRC). They fund a very wide range of projects, and those awarded since 2016 are listed here. To what extent does the HRC fund research into infectious disease?
It’s actually quite hard to tell. I pulled down two years of data from the HRC website concerning projects that were awarded funded in 2006 and 2014. Running through the list project-by-project, my estimate is that only 3% of the HRC funding in those years was allocated to researchers to study infectious disease. For the most part, HRC funding in these years mirrors the “Healthier Lives” Challenge (cancer, cardiovascular disease, diabetes and obesity) with nods to a “A Better Start” and “Aging Well”.
This week’s #InfectedNZ discussion has highlighted some of the challenges New Zealand faces from infectious disease. There is clearly concern amongst the public and amongst the scientific community about this, particularly the potential threat from antibiotic resistant bacteria. There are also significant costs to our healthcare system: as the figure below shows, we have nearly 100,000 hospital admissions per year due to infectious disease.
 It is hard to argue that a National Science Challenge in infectious disease would not have provided additionality: it would evidently have provided much needed resource in an area to which we devote less than 3% of our health research funding. If the panel that selected the National Science Challenge was correct, then it would seem we don’t have the scientific capacity in New Zealand to address infectious disease. This should be a serious concern in light of the conversation this week. Perhaps it is time to do something about it.
It is hard to argue that a National Science Challenge in infectious disease would not have provided additionality: it would evidently have provided much needed resource in an area to which we devote less than 3% of our health research funding. If the panel that selected the National Science Challenge was correct, then it would seem we don’t have the scientific capacity in New Zealand to address infectious disease. This should be a serious concern in light of the conversation this week. Perhaps it is time to do something about it.
About
Shaun Hendy is the Director of Te Pūnaha Matatini. Shaun is an advocate for multi-disciplinary research and teaching, and lectures in the University of Auckland’s Department of Physics and the University’s Centre for Innovation and Entrepreneurship.
What is InfectedNZ?
Hey, Aotearoa. It’s time we had a chat about infectious diseases and what we’re going to do about the looming antimicrobial armageddon. That’s why we’ve asked leading health, social and economic researchers, and people with personal stories, to help us get real about our vulnerability and discuss solutions. Follow their blogs right here at tepunhahamatatini.ac.nz and watch the conversation spread across social media with #infectedNZ.
Backing it all up, wherever possible, is data from the good folk at Figure.NZ. Their super duper charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #infectedNZ data board and sign-up to create your very own data board on any topic that floats your boat.

Cure Kids supporting research
At Cure Kids, we are dedicated to raising funds in order for research to be carried out that will best contribute to our vision of a healthy childhood for everyone. As the Research Manager, I am fortunate enough to have a close connection with all the research projects we fund. I’m also lucky to be able to connect with many of our wonderful ambassadors, many of whom live with the conditions that we’re researching.
In 2014, we became patently aware – via a proposal from Dr Siouxsie Wiles – about the imminent crisis that we (and by we, I mean, everyone) are facing. Over 80 years ago, health research was advanced immeasurably – and with it, health outcomes – when a beautiful collision of science and happenstance would result in the discovery of penicillin from the fungus, penicilium.
Dr Alexander Fleming, the scientist who discovered penicilium, had some ominous words, when accepting his Nobel Prize in 1945, of which we have not taken heed, ‘The thoughtless person playing with penicillin treatment is morally responsible for the death of the man who succumbs to infection with the penicillin-resistant organism’.
Dr Fleming, in equal parts wisdom and humility, knew the limitations of his momentous finding. The world has blindly careered into what may become a post-antibiotic era; to the point, now, where there are very few effective bulwarks against what were once treatable, innocuous bugs, but are now pernicious soldiers with an ever-increasing arsenal.
Antibiotics have been a great defence against unwanted visitors for decades. They have been used to prevent infections in routine surgeries, treat preterm babies, as well as provide a defence when patients undergo chemotherapy. The problem is that imprudent use is rendering antibiotics useless. We have all presumed this is a sustainable use of antibiotics; it is not.
Much like other collective-action efforts, such as action on climate change, antibiotic resistance has not been given the time of day – nor funding – it needs.
So many of our Cure Kids ambassadors have compromised immune systems, where they are vulnerable to the invasiveness of these drug-resistant bugs. Cystic fibrosis, a life-limiting inherited lung disorder is characterised by thick mucus build-up in the lungs. This mucus provides an amenable breeding ground for the bug Pseudomonas aeruginosa, with strains arising unperturbed by previous effective treatments.
A multi-pronged attack is required if we are to stave off countless deaths. While medical institutions attempt to be better stewards during prescription, Dr Wiles and her team are scouring the treasure trove of unique fungi located in New Zealand and the South Pacific. These untapped fungi could well hold a solution, and we’d like to do all we can to expedite the process of bringing the world back to an era where antibiotics are once again a powerful force against sophisticated superbugs.
Cure Kids occupy a space which deals with both the lab end, and the clinical end. We are excited to lend our support to Dr Wiles’ quest, as we are all too aware of the havoc these superbugs can wreak on our children. Us adults have reaped the benefits of advances enabled by Dr Fleming’s finding. It is now incumbent upon us to afford these same benefits to our young ones.
About
Ryan Chandler is Research Manager for Cure Kids – a charity funding vital medical research so everyone can live a healthy childhood. Donate to help.
What is InfectedNZ?
Hey, Aotearoa. It’s time we had a chat about infectious diseases and what we’re going to do about the looming antimicrobial armageddon. That’s why we’ve asked leading health, social and economic researchers, and people with personal stories, to help us get real about our vulnerability and discuss solutions. Follow their blogs right here at tepunhahamatatini.ac.nz and watch the conversation spread across social media with #infectedNZ.
Backing it all up, wherever possible, is data from the good folk at Figure.NZ. Their super duper charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #infectedNZ data board and sign-up to create your very own data board on any topic that floats your boat.
The costs of antimicrobial resistance
What might the economic costs of antibiotic/antimicrobial-resistant infections be in New Zealand? The simple answer is – we don’t know. As far as I’m aware, there’s been no New Zealand studies publicly disseminated on this topic. Therefore, we have to look overseas for reported studies.
While the US Centers for Disease Control and Prevention (2013) stated the total economic cost of antibiotic-resistant infections to the US economy was difficult to calculate, they cited year 2000 estimates provided by the Alliance for the Prudent Use of Antibiotics (APUA), an international non-governmental organisation. Based on ~900,000 cases of antibiotic-resistant infections a year, the APUA estimates ranged as high as US$20 billion in excess direct healthcare costs, with additional costs to society for lost productivity as high as US$35 billion a year. Given the number of cases reported has more than doubled over the past decade – CDC recently estimated that over 2,049,442 people are sickened every year with antibiotic-resistant infections, with at least 23,000 dying annually, who could once be easily cured – costs will have risen substantially. Furthermore, drug resistance related to viruses such as HIV and influenza was not included, nor was drug resistance among parasites such as those that cause malaria, so the true costs are likely even higher.
More recently, the UK government commissioned a review on antimicrobial resistance, in 2014, chaired by macroeconomist Jim O’Neill. As part of the two-year independent review, they estimated losses to the world economy caused by reductions to the size and efficiency of the labour force resulting from three resistant hospital-acquired infections (Escherichia coli, Klebsiella pneumoniae, and Staphylococcus aureus) and three major infectious diseases (HIV, tuberculosis, and malaria). By 2050, they projected that in a world without effective antimicrobial therapy, gross domestic product (GDP) per capita in high-income countries would be 2.3% lower each and every year compared to a world with no resistance. An older 2005 study led by the London School of Hygiene and Tropical Medicine (Richard Smith and colleagues) estimated current losses attributable to a level of MRSA (alone) of 40% in the UK at 0.4% to 1.6% of GDP – thus suggesting the review projections might be on the low side.
The review team recognised that their projected GDP losses will be an underestimation of the overall costs of antimicrobial resistance for several reasons. First, only six conditions were included as the research team was unable to identify sufficiently robust data on others. The worldwide extent of the problem is hard to pinpoint since data are incomplete, and there’s no standard for tracking such infections and associated deaths. That also makes totaling the economic impact — and exact death count — difficult to do. Second, people may choose not to undergo certain procedures because of the heightened risks involved, resulting in further morbidity and mortality. For instance, most intensive care medicine, and surgical procedures such as caesarean sections, organ transplantations, removing tumours, and hip replacements would not be possible if you don’t have effective antibiotics available that can deal with the infections that will result – modern medicine would be paralysed. And third, costs in the healthcare system and from reduced activity in travel and trade were also not included.
It’s possible we could slice and dice the costs above and apportion them to the New Zealand population. But the different methodological approaches taken, dissimilar healthcare systems, and varying usage of antibiotics in human and animal health may mean the results are not generalisable.
Given that the dangers of resistance are widely acknowledged, why hasn’t more been done in the past? One reason is that antibiotic resistance has fallen victim to evidence-based policy making, which prioritises health problems by economic burden and cost-effectiveness of interventions. While the estimated costs of antibiotic resistance are substantial, they have not been as high as in many (competing) therapeutic areas. Thus health economists have been unable to show that antibiotic resistance costs enough to be a health priority. However, the potential future costs of a world without effective antibiotics would be much larger than the cost of antimicrobial resistance today – one could draw an analogy with climate change – though it is currently not clear to what extent, or how quickly, the future burden of antimicrobial resistance will grow. The O’Neill review stated that antimicrobial-resistant infections (due to the six above conditions) are responsible for ~700,000 deaths globally each year, with this number likely to be an underestimate due to poor reporting and surveillance. By 2050, these deaths are projected to rise to 10 million a year: more than global annual cancer deaths.
International co-ordination towards the goals outlined in the Final Report and Recommendations of the Review on Antimicrobial Resistance (just published in May) is a way forward. In the words of an esteemed UK colleague, rather than see expenditure on antimicrobial policies as a cost, we should think of it as an insurance policy against a catastrophe; albeit one which we hope will never happen.
References
- US Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2013. Atlanta: CDC, Department of Health and Human Services. 2013.
- O’Neill J. Review on antimicrobial resistance. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. 2014.
- O’Neill J. The review on antimicrobial resistance. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. 2016.
- Smith RD, Yago M, Millar M, Coast J. Assessing the macroeconomic impact of a healthcare problem: The application of computable general equilibrium analysis to antimicrobial resistance. Journal of Health Economics 2005; 24(6):1055–75.
About
William Leung is a lecturer in health economics at the University of Otago, Wellington, and is currently leading the economic evaluation of SHIVERS, a CDC-funded influenza project.
What is InfectedNZ?
Hey, Aotearoa. It’s time we had a chat about infectious diseases and what we’re going to do about the looming antimicrobial armageddon. That’s why we’ve asked leading health, social and economic researchers, and people with personal stories, to help us get real about our vulnerability and discuss solutions. Follow their blogs right here at tepunhahamatatini.ac.nz and watch the conversation spread across social media with #infectedNZ.
Backing it all up, wherever possible, is data from the good folk at Figure.NZ. Their super duper charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #infectedNZ data board and sign-up to create your very own data board on any topic that floats your boat.
On the hunt for bacteriophages
The crisis of antibiotic resistant superbugs has been creeping up on us for the past 88 years. Alexander Flemming, discoverer of penicillin, the first antibiotic, in that year, said it well when he received is Nobel prize:
“It is not difficult to make microbes resistant to penicillin in the laboratory by exposing them to concentrations not sufficient to kill them, and the same thing has occasionally happened in the body. The time may come when penicillin can be bought by anyone in the shops. Then there is the danger that the ignorant man may easily underdose himself and by exposing his microbes to non-lethal quantities of the drug make them resistant.”
The superbugs that threaten to drag us back into the pre-antibiotic era today were completely predictable from the very start.
One way to think about the antibiotics is to think of them as weapons in a war that is being waged between microbes all around us. Microbes have fought for time immemorial using antibiotics and they have evolved an equally impressive cache of countermeasures: genes that confer resistance to antibiotics.
When humans stumbled into this on-going battle, we had little appreciation for the collection of resistance mechanisms that already exist in nature. To make things worse, we severely underestimate the rates that these could be borrowed or repurposed across species boundaries very easily. This is a process we now know as horizontal gene transfer.
Given our current position, looking back at the on-going microbial melee for new potential allies in this struggle is warranted. In some parts of the world, including Russia and Georgia, the natural parasites of bacteria, Bacteriophages, have been put to use in medicine since before World War I.

Bacteriophages. At left, a diagram of a typical bacteriophage. At right, A bacteriophage underneath the electron microscope.
Bacteriophages (phages for short) were discovered roughly 100 years ago, before antibiotics and they have been used medicinally in the form of small liquid vials, full of mixed cocktails of bacteriophages. Bacteriophage therapy practitioners have designed these phage cocktails and used them to great effect while the rest of Western medicine pursued Flemming’s new antibiotics.
Bacteriophages are not currently accepted in Western medicine but they are approved for use in food preparation by the USDA. Bacteriophage therapy has many obstacles to overcome before it might be accepted. One of these is the double edged sword of specificity. Bacteriophages are highly specific to a particular bacterial strain. This means that they will not hurt the beneficial microbes that contribute to our health. However it also means that finding the right one for a particular infection requires a stockpile of phage types. We need to learn more about the bacteriophages around us before we will be ready for this sort of personalized approach to fighting infection. There are estimated to be 1031 bacteriophages on the planet so as long as we can find them and study them, we have access to the stockpiles we need.
In order to learn more about these important entities, the undergraduates that take our Bacteriophage Discover and Genomics paper at Massey University are contributing to the global pool of phage information. We have joined the Howard Hughes Medical Institute’s Science Education Alliance programme to hunt for phages that are able to infect a close cousin of Mycobacterium tuberculosis. Last year we found four phages and sequenced two. As far as we know these are the very first Mycobacteriophages to be found in New Zealand (below figure).

Phage Hunt Map. Each symbol represents a single sequenced Mycobacteriophage. Last year, the phage hunters at Massey University put NZ on the map!
To hear more about Bacteriophages, watch Heather’s TedX talk.
It’s an exciting time to be a phage hunter! To learn more about our phage hunt, check out the student blog, Phage Hunt NZ.
About
 Dr Heather Hendrickson is a Senior Lecturer at Massey University. She has been dabbling in Phage Hunting since her time at the Pittsburgh Bacteriophage Institute as a PhD student. Heather’s laboratory at Massey University, Auckland studies the evolution of bacteria and bacteriophage discovery in Pseudomonas, Mycobacteria and Lactococcus.
Dr Heather Hendrickson is a Senior Lecturer at Massey University. She has been dabbling in Phage Hunting since her time at the Pittsburgh Bacteriophage Institute as a PhD student. Heather’s laboratory at Massey University, Auckland studies the evolution of bacteria and bacteriophage discovery in Pseudomonas, Mycobacteria and Lactococcus.
What is InfectedNZ?
Hey, Aotearoa. It’s time we had a chat about infectious diseases and what we’re going to do about the looming antimicrobial armageddon. That’s why we’ve asked leading health, social and economic researchers, and people with personal stories, to help us get real about our vulnerability and discuss solutions. Follow their blogs right here at tepunhahamatatini.ac.nz and watch the conversation spread across social media with #infectedNZ.
Backing it all up, wherever possible, is data from the good folk at Figure.NZ. Their super duper charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #infectedNZ data board and sign-up to create your very own data board on any topic that floats your boat.
The 3Rs of antimicrobial resistance: going back to basics to avert a crisis
Down in Otago, researchers’ focus on microbiology fundamentals is leading New Zealand’s fight against drug resistant pathogens.
In May 2016 the UK government’s Review on Antimicrobial Resistance (AMR) published its final report, summarising the Review’s findings from two years of analysis. The conclusions, whilst welcomed by the scientific community, chimed with what leading researchers, such as the University of Otago’s Professor Greg Cook, have more or less been saying for over a decade. Namely, that AMR is already a global problem (including here in Aotearoa New Zealand) and that it will take a concerted effort with governments, scientists and pharmaceutical companies working together to solve it. In the meantime the report recommended taking steps that could help prevent the rise and spread of AMR. These, in essence, can be boiled down to the three R’s of antimicrobials: Refine, Reduce and Replace, and it is these three R’s that research in Prof Cook’s laboratory focuses on.
Refining the use of antibiotics basically means using the right drugs, to treat the right bugs, at the right time. In order to achieve that, healthcare workers need rapid diagnostic tests which will tell them whether the bug their patient has is already resistant to antibiotics, and if so, to which ones. The Cook lab is part of an international collaboration between Otago and South East Asia whereby the team is trying to establish whole genome sequencing (WGS) of the tuberculosis (TB)-causing bacterium, Mycobacterium tuberculosis, as a route to faster diagnoses. WGS allows researchers to analyse the genome of AMR bacteria, looking for genetic markers that indicate which antibiotics will work and those to which the bacterium is resistant.
The second of the three R’s, Reduce, is aimed at using fewer antibiotics to lower levels of AMR in our society and in the environment. An unfortunate Catch 22 experienced in antibiotic use is that, the more you use an antibiotic, the faster resistance will arise. Around the world there are many countries that use huge numbers of antibiotics in farming. In the Unites States alone roughly 70% of antimicrobials used each year are used on animals. Luckily for us, New Zealand is one of the lowest users of antibiotics in farming worldwide but still, there’s room for improvement.
In the dairy industry, when a cow’s udder becomes infected (know as mastitis) it’s more often than not due to a bacterial infection and treatment involves a course of antibiotics, such as penicillin. Moreover, whenever a cow is treated with antibiotics its milk can’t be used and needs to be discarded. Treatment and discarded milk cost the New Zealand dairy industry over $280 million a year. In this scenario, prevention really is better than the cure, for all of us. By joining forces with a leading animal remedy company, Deosan, as well as chemists from the University of Auckland, Prof Cook and co-lead investigator Dr Adam Heikal are heading up a team dedicated to finding new bio-active, sanitising molecules to help stop dairy herds developing mastitis in the first place, thereby reducing the farmers’ antibiotic needs.
Sanitisers for dairy cows are already widely used but the bioactive molecules they contain are also used extensively in hospitals across the country and around the world. To reduce the chances of resistance to these molecules arising on the farm, and spreading to the clinic it’s vital the new molecules, specifically for farm use, are discovered and developed. That forms one part of the final R, Replace.
The search for new antimicrobials is a never-ending one. As fast as new drugs are discovered, resistance starts to evolve. For this reason, the Cook lab invests heavily in screening large libraries of chemical compounds and natural products against problem bacteria, looking for new antimicrobial drug targets. However whole organisms, even those as small as a bacterial cell, are extremely complex. To reduce the levels of complexity, once a new antimicrobial target is identified, using either reverse genetics or a good old-fashioned experimental process of elimination, the target can be purified away from the organism and studied in greater detail. Three-dimensional structures can guide researchers to make more potent, more specific drugs. Recently, the Cook lab published the first bacterial structure of a protein long thought to be a drug target for tuberculosis treatment. The challenge now is to understand, at a molecular level, the enzyme’s inner workings and to ultimately inhibit its mode of action, leading to the design of a new antimicrobial drug.
The combination of all these research activities, as well as extensive international and industrial collaborations, help the Cook lab keep New Zealand at the forefront of antimicrobial discovery.
Check out some of the data about tuberculosis and vaccinations for whooping cough from the Figure.NZ team:
https://figure.nz/chart/0tUNDA6VMX0x6W5z
https://figure.nz/chart/AzwxPvVYJbh0lrcY-7fKh6eHZQCbjqKme
InfectedNZ data board: https://figure.nz/@InfectedNZ/public
About
Adam Heikal PhD is a former Research Fellow in the Department of Microbiology and Immunology, University of Otago. He continues to work in AMR and antimicrobial discovery at the School of Pharmacy, University of Oslo and remains in close collaboration with Prof Cook as co-Principal Investigator on projects related to the New Zealand Agritech sector. Follow Adam on LinkedIn.
What is InfectedNZ?
Hey, Aotearoa. It’s time we had a chat about infectious diseases and what we’re going to do about the looming antimicrobial armageddon. That’s why we’ve asked leading health, social and economic researchers, and people with personal stories, to help us get real about our vulnerability and discuss solutions. Follow their blogs right here at tepunhahamatatini.ac.nz and watch the conversation spread across social media with #infectedNZ.
Backing it all up, wherever possible, is data from the good folk at Figure.NZ. Their super duper charts are based on data sourced from public repositories, government departments, academics and corporations. Check out their #infectedNZ data board and sign-up to create your very own data board on any topic that floats your boat.